

Thyroid cancer is a cancer that starts in the thyroid gland. To understand thyroid cancer, it helps to know about the normal structure and function of the thyroid gland.
The thyroid gland:
The thyroid gland is under the thyroid cartilage (Adam's apple) in the front part of the neck. In most people, the thyroid cannot be seen or felt. It is butterfly shaped, with 2 lobes-- the right lobe and the left lobe-- joined by a narrow isthmus (see picture below).
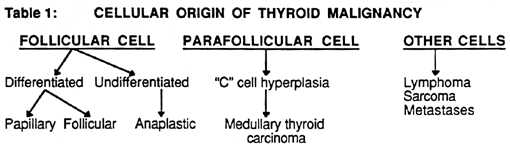
The thyroid gland contains mainly 2 types of cells: thyroid follicular cells and C cells (also called parafollicular cells).
The follicular cells use iodine from the blood to make thyroid hormone, which helps regulate a person's metabolism.
Too much thyroid hormone (a condition called hyperthyroidism) can cause a rapid or irregular heartbeat, trouble sleeping, nervousness, hunger, weight loss, and a feeling of being too warm.
Too little hormone (called hypothyroidism) causes a person to slow down, feel tired, and gain weight. The amount of thyroid hormone released by the thyroid is regulated by the pituitary gland at the base of the brain, which makes a substance called thyroid-stimulating hormone (TSH).
C cells (parafollicular cells) make calcitonin, a hormone that helps regulate how the body uses calcium.
Other, less common cells in the thyroid gland include immune system cells (lymphocytes) and supportive (stromal) cells.
Different cancers develop from each kind of cell. The differences are important because they affect how serious the cancer is and what type of treatment is needed.
Many types of tumors can develop in the thyroid gland. Most of them are benign (non-cancerous) but others are malignant (cancerous), which means they can spread into nearby tissues and to other parts of the body.
Benign thyroid enlargement and nodules:
Because the thyroid gland is right under the skin, changes in its size and shape can often be felt or even seen by patients or by their doctor.
The medical term for an abnormally large thyroid gland is goiter. Some goiters are diffuse, meaning that the whole gland is large. Other goiters are nodular, meaning that the gland is large and has one or more bumps in it. There are many reasons the thyroid gland might be larger than usual, and most of the time it is not cancer. Both kinds of goiter are usually caused by an imbalance in certain hormones. For example, not getting enough iodine in the diet can cause changes in hormone levels and lead to a goiter.
Lumps or bumps in the thyroid gland are called thyroid nodules. Most thyroid nodules are benign, but about 1 in 20 is cancerous (see the next section).
People can develop thyroid nodules at any age, but they are most common in older adults. Fewer than 1 in 10 adults have thyroid nodules that can be felt by a doctor. But when the thyroid is looked at with an ultrasound test, up to half of all people are found to have nodules that are too small to feel.
Most nodules are cysts filled with fluid or with a stored form of thyroid hormone called colloid. Colloid nodules are one of the most common types of thyroid nodule.
Solid nodules have little fluid or colloid. Some solid nodules may have too many cells, but the cells are not cancer cells. These types of nodules include hyperplastic nodules and adenomas. Sometimes these nodules make too much thyroid hormone and cause hyperthyroidism.
Benign thyroid nodules can sometimes be left alone (not treated) as long as they're not growing or causing symptoms. Others may require some form of treatment.
Malignant thyroid tumors:
Only about 1 in 20 thyroid nodules is cancerous. The 2 most common types of thyroid cancer are called papillary carcinoma and follicular carcinoma. Hürthle cell carcinoma is a subtype of follicular carcinoma. All these types are differentiated tumors.
There are some other types of thyroid cancer, such as medullary thyroid carcinoma, anaplastic carcinoma, and thyroid lymphoma, but these occur less often.
Differentiated thyroid cancers:
Differentiated thyroid cancers develop from thyroid follicular cells. In these cancers, the cells appear similar to normal thyroid tissue when looked at under a microscope.
Papillary carcinoma:
About 8 of 10 thyroid cancers are papillary carcinomas (also called papillary cancers or papillary adenocarcinomas). Papillary carcinomas typically grow very slowly. Usually they develop in only one lobe of the thyroid gland, but sometimes they occur in both lobes. Even though they grow slowly, papillary carcinomas often spread to the lymph nodes in the neck. But most of the time, this can be successfully treated and is rarely fatal.
Several different variants (subtypes) of papillary carcinoma can be recognized under the microscope. Of these, the follicular variant (also called mixed papillary-follicular variant) occurs most often.
The usual form of papillary carcinoma and the follicular variant have the same outlook for survival (prognosis), and are treated the same.
Other variants of papillary carcinoma (columnar, tall cell, diffuse sclerosis) are not as common and tend to grow and spread more quickly.
Follicular carcinoma:
Follicular carcinoma is the next most common type of thyroid cancer. It is also sometimes called follicular cancer or follicular adenocarcinoma. Follicular cancer is much less common than papillary thyroid cancer, making up about 1 out of 10 thyroid cancers.
It is more common in countries where people don't get enough iodine in their diet. These cancers usually remain in the thyroid gland. Unlike papillary carcinoma, follicular carcinomas usually don't spread to lymph nodes, but some can spread to other parts of the body, such as the lungs or bones.
The prognosis for follicular carcinoma is probably not quite as good as that of papillary carcinoma, although it is still very good in most cases.
Hürthle cell carcinoma, also known as oxyphil cell carcinoma, is actually a kind of follicular carcinoma. This type accounts for about 3% of thyroid cancers. The prognosis may not be as good as that of typical follicular carcinoma because this subtype is harder to find and treat as it is less likely to absorb radioactive iodine.
Radioactive iodine is used for treatment and to find metastases of differentiated thyroid cancer.
Other types of thyroid cancers
Medullary thyroid carcinoma:
Medullary thyroid carcinoma (MTC) accounts for about 4% of thyroid cancers. It develops from the C cells of the thyroid gland. Sometimes this cancer can spread to lymph nodes, the lungs, or liver even before a thyroid nodule is discovered. These cancers usually release calcitonin and carcinoembryonic antigen (CEA) into the blood, causing high levels of these when checked by blood tests.
Calcitonin is a hormone that helps control the amount of calcium in blood. CEA is a protein made by certain cancers, such as colorectal cancer and MTC. Because medullary cancer does not absorb or take up radioactive iodine (used for treatment and to find metastases of differentiated thyroid cancer), the prognosis (outlook) is not quite as good as that for differentiated thyroid cancers.
There are 2 types of MTC.
The first type, occurring in about 8 of 10 cases, is called sporadic MTC. Sporadic MTC is not inherited; that is, it does not run in families. It occurs mostly in older adults and affects only one thyroid lobe.
The other type of MTC is inherited and can occur in each generation of a family. These familial MTCs often develop during childhood or early adulthood and can spread early. Patients usually have cancer in both thyroid lobes and in several areas of each lobe. They are often linked with an increased risk of other types of tumors.
Anaplastic carcinoma:
Anaplastic carcinoma (also called undifferentiated carcinoma) is a rare form of thyroid cancer, making up about 2% of all thyroid cancers. It is thought to sometimes develop from an existing papillary or follicular cancer. This cancer is called undifferentiated because the cancer cells do not look very much like normal thyroid tissue cells under the microscope. This is an aggressive cancer that rapidly invades the neck, often spreads to other parts of the body, and is very hard to treat.
Thyroid lymphoma:
Lymphoma is very uncommon in the thyroid gland. Lymphomas are cancers that develop from lymphocytes, the main cell type of the immune system. Most lymphocytes are found in lymph nodes, which are pea-sized collections of immune cells scattered throughout the body (including the thyroid gland).
Thyroid sarcoma:
These rare cancers start in the supporting cells of the thyroid. They are often aggressive and hard to treat.
Parathyroid cancer:
Behind, but attached to, the thyroid gland are 4 tiny glands called the parathyroids. The parathyroid glands help regulate the body's calcium levels. Cancers of the parathyroid glands are very rare -- there are probably fewer than 100 cases each year in the United States.
Parathyroid cancers cause the blood calcium level to be elevated. This causes a person to become tired, weak, and drowsy. High calcium also makes you urinate (pee) a lot causing dehydration, which can make the weakness and drowsiness worse. Other symptoms include bone pain and fractures, pain from kidney stones, depression, and constipation.
Larger parathyroid cancers may also be found as a nodule near the thyroid. No matter how large the nodule is, the only treatment is to remove it surgically. Unfortunately, parathyroid cancer is much harder to cure than thyroid cancer. The remainder of this document only discusses thyroid cancer.

Last Medical Review: 05/12/2010
Last Revised: 07/20/2010

No comments:
Post a Comment